Hyperthermie
Mit Fieber und Wärme behandeln
Was ist Hyperthermie?
Die Behandlung mit Hyperthermie beruht auf einer gezielten Erwärmung des Körpers oder einzelner Körperpartien. Durch den dabei entstehenden «Hitzestress» werden die Krebszellen empfindlicher gegenüber körpereigenen Abbauprozessen, einer begleitenden Strahlenbehandlung oder Chemotherapie. Ziel der verschiedenen Hyperthermie-Verfahren ist es jedoch nicht, die Krebszellen durch die Wärme direkt abzutöten.
Im Zentrum für Integrative Onkologie werden die moderate Ganzkörper-Hyperthermie und die passive lokale Tiefenhyperthermie angeboten. Ein weiteres Verfahren ist die aktive Fiebertherapie. Mehr Informationen zu diesem Verfahren siehe Flyer «Misteltherapie». Unser Zentrum ist Gründungsmitglied des Swiss-Hyperthermia-Network. Alle Mitglieder dieses Netzwerks sind verpflichtet, gemäss den Qualitätsstandards der European Society for Hyperthermic Oncology (ESHO) zu behandeln.
Weitere Infos
Hyperthermie im Zusammenhang mit Chemotherapie: Bessere Verteilung von Zytostatika
Durch die Behandlung mit Hyperthermie erwärmt sich das bestrahlte Körpergewebe. Die Blutgefässe weiten sich und führen zu einer stärkeren Durchblutung des Tumors. So gelangen nun auch in ursprünglich schlecht durchblutete Tumoranteile grössere Mengen an Chemotherapie-Medikamenten. Dadurch kann ihre Wirkung auf Krebszellen verbessert werden, die unter normalen Temperaturen nur schlecht auf die Behandlung ansprechen würden, weil sie zum Beispiel im Inneren sehr grosser Tumoren liegen. Zudem nehmen die Krebszellen selbst bei Hitze durch ihren beschleunigten Stoffwechsel mehr Zytostatika auf. Hinzu kommt ausserdem eine Schädigung der zelleigenen Reparaturmechanismen durch die Hyperthermie.
Hitzeschockproteine: Signal für das Immunsystem
Bei lang andauernder und/oder wiederholter Behandlung mit Hyperthermie bilden Körperzellen sogenannte Hitzeschockproteine, auch «Stresseiweisse» genannt. Diese Eiweisse wirken als Signale für die körpereigen Abwehr und aktivieren sogenannte «Killerzellen», die für den Abbau von Krebszellen zuständig sind.
Strahlentherapie und Überwärmung
Blutgefässe innerhalb von Tumoren sind oft weniger geordnet angelegt, als dies in gesundem Körpergewebe der Fall ist. Auch kann die Entwicklung der Blutgefässe bei manchen Tumoren nicht mit dem schnellen Wachstum der Krebszellen Schritt halten. Als Folge finden sich in grösseren Tumoren häufig Bereiche, die schlecht mit Sauerstoff versorgt sind. Die Krebszellen in diesen Regionen sind meist weniger anfällig für eine Strahlentherapie, reagieren aber vergleichsweise empfindlich auf eine Überwärmung. Durch die Verbindung von Hyperthermie und Bestrahlung soll somit erreicht werden, dass die Zellen, die eine Strahlentherapie überstehen, stattdessen durch die Hitze geschädigt werden – die Wirkung beider Therapien addiert/ergänzt sich. Zudem verbessert die Hyperthermie mit der Durchblutung auch die Sauerstoffversorgung des Krebsgewebes Auf diese Weise entstehen unter der Bestrahlung mehr sogenannte «Sauerstoffradikale», die Krebszellen beschädigen können. Hinzu kommt in der Folge auch hier, dass unter hohen Temperaturen die Reparaturmechanismen der Zellen versagen: Die Krebszellen können die durch die Bestrahlung und die Sauerstoffradikale entstandenen Schäden nicht mehr oder nur noch in sehr geringem Masse kompensieren und gehen zugrunde.
Publikationen und Studien
Das ZIO ist Netzwerkmitglied des Swiss Hyperthermia Network. Im 2015 gegründeten Swiss Hyperthermia Network haben sich schweizweit 15 Partnerkliniken zusammengeschlossen, um potenziellen Patientinnen und Patienten in der Schweiz einen Zugang zur Hyperthermie-Behandlung zu ermöglichen. Ziel des Netzwerkes ist eine evidenzbasierte, interdisziplinäre Indikationstellung für alle Patientinnen und Patienten. Die Partnerkliniken führen wöchentlich ein virtuelles Hyperthermie-Tumorboard durch.
Laufende Studien
Ongoing Clinical Trials in Hyperthermia at KSA-KSB
1. Muscle invasive bladder cancers
September 2012 – ongoing
A phase IIB study of the tetramodal therapy of T2-4NxM0 bladder cancer with hyperthermia combined with chemoradiotherapy following TUR-BT. (PI: Dr. B. Eberle / Dr. E. Puric, KSA).
End point
Primary: CR at end of treatment / Secondary: Functional bladder preservation, PFS and OS.
2. Soft tissue sarcoma
October 2013 – ongoing till 2018
A phase I/II study of concurrent hyperthermia and proton beam radiotherapy in primary and recurrent unresectable soft tissue sarcoma. (PI: Prof. N.R. Datta, KSA). ClinicalTrials.gov NCT01904565.
End point
Primary: Local tumour control, Acute and late morbidity, wound complication / Secondary: Local control rate at 2 years, LDFS at 2 years.
3. Locally advanced pancreatic cancers
August 2016 – till 2021
A randomized phase II study of concurrent hyperthermia and chemoradiotherapy following neoadjuvant chemotherapy in locally advanced pancreatic cancers (HEATPAC). (PI: Prof. N.R. Datta, KSA). ClinicalTrials.gov NCT02439593.
End point
Primary: OS at 1 year, Acute and late morbidities / Secondary: Patterns of failure, PFS, DFS and OS.
4. Inoperable Chordomas
June 2016 – ongoing
Phase I/II feasibility study with hyperthermia and proton beam radiotherapy in inoperable chordomas. Sponsors: PSI, KSA-KSB.
End point
Primary: Feasibility Secondary: Response rates, subjective improvement in symptoms.
Ongoing Clinical Trials in Hyperthermia at Germany, Netherlands and Poland with hyperthermia
1. Soft tissue sarcoma
July 2015 – July 2018
Trabactedin combined with regional hyperthermia as second line treatment for adult patients with advanced soft tissue sarcoma. Sponsors: Ludwig-Maximilians University of Munich, Klinikum Großhadern (Prof. R. Issels, Prof. Lars Linder). ClinicalTrials.gov NCT02359474.
End point
Primary: Progression free survival / Secondary: Overall survival.
2. Locally recurrent head and neck cancers
March 2017 – Feb 2022
HyBT-H&N: Salvage brachytherapy with interstitial hyperthermia for locally recurrent head & neck carcinoma following previously external beam radiation therapy. Sponsors: University Klinik of Erlangen, Germany (Prof. V. Strnad, Prof. R. Fitkau).
End point
Primary: Loco-regional control (salvage) / Secondary: Acute and late morbidity.
3. Invasive bladder cancers
Feb 2017 – Jan 2022
HyBla-RCT: Organ preservation treatment in bladder cancers with chemoradiotherapy vs thermochamoradiotherapy. Sponsors: University Klinik of Erlangen, Germany.
End point
Primary: Loco-regional control / Secondary: Bladder preservation, Relapse free survival (local and distant), acute and late toxicity.
4. Cancer cervix
Submitted for Ethical approval June 2017
HyZer_RCT_IBT: Multimodality therapy with chemoradiotherapy versus thermochemoradiotherapy and interstitial thermobrachytherapy.
End point
Primary: Overall survival / Secondary: Relapse free survival (local and distant), acute and late toxicity.
5. Recurrent prostate cancer
Jan 2015
Regional hyperthermia and moderately dose-escalated salvage radiotherapy for recurrent prostate cancer: A phase II study. Sponsors: Charité, University Klinik Berlin, University Klinik of Tübingen (Dr. P. Ghajar).
End point
Primary: Acute GU toxicity.
6. Recurrent prostate cancer
May 2015 – ongoing
Prostate BT-HT: A prospective phase II study of salvage brachytherapy in combination with interstitial hyperthermia for locally recurrent prostate carcinoma following external beam radiation therapy. Sponsors: M.Sklodowskiej-Curie, Krakow, Poland and University Klinik of Erlangen (Dr.A. Kukielka, Dr. V. Strnad).
End point
Primary: Loco-regional control / Secondary: acute and late toxicity.
7. Resected pancreatic cancers
Sept 2013 – ongoing
A randomized two-armed open study on the adjuvant therapy in patients with R0/R1 resected pancreatic carcinoma with Gemcitabine plus Capecitabine (Arm GC) vs. Gemcitabine plus Cisplatin with regional hyperthermia (Arm GPH). Sponsors: Klinikum Grosshadern, Medical Center, University of Munich (Dr. K. Lechner, Prof. L. Linder, Prof. R. Issels). HEAT-Study EudraCT-Nr.: 2008-004802-14. ClinicalTrials.gov NCT01077427.
End point
Primary: Disease free survival / Secondary: Overall survival, acute and late toxicity.
8. Locally recurrent rectal cancers
March 2011 – ongoing
Neoadjuvant chemoradiation with 5-FU and Oxaliplatin combined with deep regional hyperthermia in locally recurrent rectal cancer. A multi-institutional Phase I/II Study (HyRec Trial). Sponsors: University Klinik of Erlangen, Germany (Prof. O.Ott, Prof. R. Fietkau). HyRec Trial Strahlenklinik 2009-010093-38. ClinicalTrials.gov NCT01716949.
End point
Primary: Feasibility rate / Secondary: Local progression-free survival, Distant metastasis-free survival (excluding M1 patients), Overall survival (excluding M1 patients), Response rate (RECIST criteria), Rate of curative resections (R0), Rate of acute and late toxicity.
9. Anal cancers
Dec 2014 – April 2021
Phase 2 Randomized Trial to evaluate effects of deep regional hyperthermia in patients with anal carcinoma treated by standard radiochemotherapy (Hycan). Sponsors: University of Erlangen-Nürnberg Medical School (Dr. G. Grabenbauer). ClinicalTrials.gov NCT02369939.
End point
Primary: Improvement of complete remission / Secondary: Colostomy-free survival, Locoregional relapse-free survival , Overall relapse-free survival, Overall survival, Response rate, Acute and late toxicity, Quality of life.
10. Localized prostate cancers
Presently not active
Prospective randomized phase III trial comparing postsurgical radiotherapy alone versus adjuvant radiotherapy plus hyperthermia in patients with localized prostate cancer. Sponsors: Akademisches Lehrkrankenhaus Radiologie- Zentrum of Fulda, Germany, Univ Hospital Verona, Italy (Dr. H.J. Feldmann, Prof. S. Maluta).
End point
Primary: Freedom from progression / Secondary: local-regional progression, distant metastases, disease-free survival, prostate cancer specific survival, nonprostate cancer specific survival, overall survival, and time to biochemical (PSA) failure, acute and late toxicity.
11. Muscle invasive bladder cancers
Details NA
Chemoradiation plus hyperthermia in muscle invasive bladder cancer: A phase II trial. (PI: M. Hulshof, Amsterdam).
End point
Details : NA.
12. Locally advanced rectal cancer
June 2018 – April 2024
Organ preservation in locally advanced rectal cancer by radiochemotherapy followed by consolidation chemotherapy (CAO/ARO/AIO-16). Sponsors / Collaborators: University Hospital Tübingen, Germany. ClinicalTrials.gov NCT03561142.
End point
Primary: Clinical complete response / Secondary: Local regrowth rate, safety, faecal incontinence, QOL, surgical interventions, surgical morbidity, pathological staging, R0 rate, Rate of sphincter sparing surgery, relapse free survival, overall survival.
Relevant Clinical Trials worldwide listed in clinicaltrials.gov on hyperthermia for selected sites as on Jan’2020
1. Cancer cervix
Recruiting
Modulated Electro-Hyperthermia plus Chemo-radiation for locally Advanced Cervical Cancer patients in South Africa. Interventions – Device: Modulated electro-hyperthermia / Radiation: External beam radiation / Drug: Cisplatin / Radiation: Brachytherapy.
Locations
Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, Gauteng, South Africa.
2. Rectal Cancer
Active, not recruiting
The Effect of Electro-Hyperthermia in Preoperative Radiotherapy for Locally Advanced Rectal Cancer. Interventions – Device: Electrohyperthermia.
Locations
Wonju Severance Christian Hospital, Wonju, Gangwon, Korea, Republic of.
3. Rectal Cancer
Recruiting
Neoadjuvant Chemoradiation with 5-FU(or Capecitabine) and Oxaliplatin Combined with Hyperthermia in Rectal Cancer. Interventions – Radiation: Radiotherapy / Procedure: Hyperthermia / Drug: 5-Fluorouracil / Drug: Capecitabine / Drug: Oxaliplatin.
Locations
Klinik Bad Trissl, Innere Medizin, Bad Trissl, Germany / University Hospital, Duesseldorf, Germany / Universitätsklinikum Erlangen, Strahlenklinik, Erlangen, Germany / LMU München, Campus Großhadern, Medizinische Klinik III, Hyperthermie, München, Germany / Schlossbergklinik, Oberstaufen, Germany / Universitätsklinikum Tübingen, Radioonkologie, Tübingen, Germany.
4. Locally Advanced Rectal Cancer
Terminated
Efficacy of NeoThermo-Radiochemotherapy for LA Rectal Cancer Before Laparoscopic TME: Prospective Phase II Trial. Interventions – Radiation: Hyperthermia with concurrent chemo-radiation therapy.
Locations
Samsung Medical Center, Seoul, Korea, Republic of.
5. Locally Advanced Rectal Cancer
Completed
Preoperative Radiochemotherapy with Hyperthermia for locally advanced Rectal Cancer. Interventions – Hyperthermia / Hyperthermic Radiochemotherapy / Hyperthermic Chemoradiotherapy / Deep Regional Hyperthermia / Other: Deep regional hyperthermia / Radiation: Radiotherapy / Drug: Chemotherapy (5-Fluorouracil).
Locations
University Hospital Tübingen, Department of Radiation Oncology, Tübingen, Baden-Württemberg, Germany.
6. Rectal Cancer
Recruiting
Organ Preservation in Locally Advanced Rectal Cancer by Radiochemotherapy Followed by Consolidation Chemotherapy. Interventions – Radiation: Radiotherapy / Drug: Chemotherapy / Other: Deep regional hyperthermia.
Locations
University Hospital Erlangen, Erlangen, Germany / University Hospital Frankfurt, Frankfurt, Germany / University Hospital Tübingen, Tübingen, Germany / University Hospital Würzburg, Würzburg, Germany.
7. Soft Tissue Sarcoma
Ongoing
Hyperthermia and Proton Therapy in Unresectable Soft Tissue Sarcoma. Interventions – Radiation: Hyperthermia and Proton Beam.
Locations
Kantonsspital Aarau, Aarau, Aargau, Switzerland / PSI, Viilligef / Univ Hosp Zurich /Balgrist Clinic, Zurich.
8. Sarcoma
Completed
Combination Chemotherapy with or without Hyperthermia Therapy in Treating Patients with Soft Tissue Sarcoma. Interventions – Drug: doxorubicin hydrochloride / Drug: etoposide / Drug: ifosfamide / Procedure: conventional surgery / Procedure: hyperthermia treatment / Radiation: radiation therapy.
Locations
Robert Roessle Comprehensive Cancer Center at University of Berlin – Charite Campus Buch, Berlin, Germany / Universitaetsklinikum Essen, Essen, Germany / Universitaetsklinikum Hamburg-Eppendorf, Hamburg, Germany / Klinikum der Universitaet Muenchen – Grosshadern Campus, Munich, Germany.
9. Sarcoma, Alveolar Soft Part Sarcoma, Clear Cell Sarcoma, Malignant Peripheral Nerve Sheath Tumors, Myxoid Liposarcoma, Liposarcoma, Dedifferentiated, Synovial Sarcoma, Leiomyosarcoma, Undifferentiated Pleomorphic Sarcoma, Fibrosarcoma, Pleomorphic Rhabdomyosarcoma
Recruiting
Preoperative Hypofractionated Radiotherapy with Hyperthermia in Unresectable or Marginally Resectable Soft Tissue Sarcomas. Interventions – Radiation: Hypofractionated radiotherapy / Other: Hyperthermia.
Locations
Maria Sklodowska-Curie Institute – Oncology Center, Warsaw, Mazovian, Poland.
10. Sarcoma
Recruiting
Hyper-Thermia Enhanced Antitumor Efficacy of Trabectedin. Interventions – Drug: Trabectedin / Genetic: DNA doublestrand breaks / Hyperthermia.
Locations
Ludwig-Maximilians University of Munich, Klinikum Großhadern, Munich, Bavaria, Germany / Helios Klinikum Bad Saarow, Bad Saarow, Germany / Charité – Universitätsmedizin Berlin, Berlin, Germany / Helios Klinikum BerlinBuch, Berlin, Germany / Universitätsklinikum Erlangen, Erlangen, Germany.
11. Pancreatic Neoplasms
Unknown status
Hyperthermia with Chemotherapy for Locally Advanced or Metastatic Pancreas Cancer. Interventions – Device: Heckel Infrared Radiant Heat Device / Other: cisplatin, gemcitabine, interferonalpha / Other: thermochemotherapy.
Locations
Memorial Hermann Hospital, Houston, Texas, United States.
12. Cancer Pancreas
Unknown status
Multicenter RCT of the Clinical Effectiveness of Oncothermia with Chemotherapy in Metastatic Pancreatic Cancer Patients. Interventions – Other: Oncothermia / Drug: FOLFIRINOX or Gemcitabine based chemotherapy.
Locations
Seoul National University Bundang Hospital, Seongnam, Gyeonggi-do, Korea, Republic of.
13. Cancer Pancreas
Recruiting
Concurrent Hyperthermia and Chemoradiotherapy in LAPC: Phase II Study. Interventions – Other: Chemoradiotherapy (CTRT) / Other: Thermochemoradiotherapy (CTRTHT).
Locations
Kantonsspital Aarau, Aarau, Aargau, Switzerland.
14. All Type of Cancers with Bony Metastasis.
Unknown status
Comparing the Effectiveness of Combined Hyperthermia and External Beam Radiation (EBRT) Versus EBRT Alone in Treating Patients with Painful Bone Metastases. Interventions – Other: Hyperthermia / Radiation: External-beam radiotherapy.
Locations
Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan.
Aktuelle Publikationen
Current indications of deep hyperthermia at Kantonsspital Aarau with levels of evidence for each site and the related key citations
Indication: Cervix-Ca
- Hyperthermia and radiotherapy with or without chemotherapy in locally advanced cervical cancer: A systematic review with conventional and network meta-analyses. Datta NR, Rogers S, Klingbiel D, et al. Int J Hyperthermia 2016 (in press).
- Combined use of hyperthermia and radiation therapy for treating locally advanced cervix carcinoma. Lutgens L, van der Zee J, Pijls-Johannesma M, et al. Cochrane Database Syst Rev. 2010:CD006377.
- Long-term improvement in treatment outcome after radiotherapy and hyperthermia in locoregionally advanced cervix cancer: an update of the Dutch Deep Hyperthermia Trial. Franckena M, Stalpers LJ, Koper PC, et al. Int J Radiat Oncol Biol Phys. 2008;70:1176-82.
- HDR brachytherapy combined with interstitial hyperthermia in locally advanced cervical cancer patients initially treated with concomitant radiochemotherapy–a phase III study. Zolciak-Siwinska A, Piotrkowicz N, Jonska-Gmyrek J, et al. Radiother Oncol 2013;109:194-9.
- A randomized clinical trial of radiation therapy versus thermoradiotherapy in stage IIIB cervical carcinoma. Harima Y, Nagata K, Harima K, et al. Int J Hyperthermia 2001;17:97-105.
- Local thermo-radiotherapy in carcinoma cervix: Improved local control versus increased incidence of distant metastasis. Sharma S, Singhal S, Sandhu AP, et al. Asia Oceania J Obstet Gynaecol 1991;17:5-12.
- Thermoradiotherapy in the management of carcinoma cervix (stage IIIB): a controlled clinical study. Datta NR, Bose AK, Kapoor HK. Indian Med Gazette 1987;121: 68-71.
- A randomized trial of hyperthermia-radiochemotherapy for uterine cervix cancer. Chen HW, Fan JJ, Luo W. Zhonghua Zhong Liu Za Zhi 1997;24:249-51.
- A multicentre randomised clinical trial of chemoradiotherapy plus hyperthermia versus chemoradiotherapy alone in patients with locally advanced cervical cancer. Harima Y, Ohguri T, Imada H et al. Int J Hyperthermia. 2016 Nov;32(7):801-8.
- Radiation therapy combined with hyperthermia versus cisplatin for locally advanced cervical cancer: Results of the randomized. Lutgens LC, Koper PC, Jobsen JJ et al. J.radonc.2016.02.010.
- Network meta-analysis in locally advanced cervical cancer: evaluation of outcomes with chemoradiation therapy or thermoradiation therapy versus radiation therapy alone. Datta NR, Rogers S, Hutton B, et al. Int J Radiat Oncol Biol Phys 2016; 96(2), E324.
- Hyperthermia and radiotherapy with or without chemotherapy in locally advanced cervical cancer: A systematic review with conventional and network meta-analysis. Datta NR, Rogers S, Klingbiel D, et al. SASRO 2016. (Awarded Best paper) Strahlenther Oncol 2016;192:832.
- Does hyperthermia with radiotherapy / chemoradiotherapy offer a therapeutic advantage in inoperable locally advanced cervix cancer? : A systematic review and network meta-analysis. Datta NR, Stutz E, Gomez S, et al. ESHO Berlin, 16-18 May 2018 (Oral presentation)
- Systematic review & network meta-analysis to identify the optimum nonoperative therapeutic strategies in locally advanced cancer cervix. Datta NR, Stutz E, Gomez S, Bodis S. SASRO 2018
- Therapeutic Options for Locally Advanced Cancer Cervix: A Systematic Review and Network Meta-analysis. Datta NR, Stutz E, Gomez S, Bodis S.. (Accepted for presentation), ASTRO 2018, San Antonio, Texas, USA.
- The effect of modulated electrohyperthermia on local disease control in HIV-positive and -negative cervical cancer women in South Africa: Early results from a phase III randomised controlled trial. Minnaar CA, Kotzen JA, Ayeni OA, et al. PLoS One 2019;14:e0217894.
- Efficacy and Safety Evaluation of the Various Therapeutic Options in Locally Advanced Cervix Cancer: A Systematic Review and Network Meta-Analysis of Randomized Clinical Trials. Datta NR, Stutz E, Gomez S, Bodis S. Int J Radiat Oncol Biol Phys 2019;103:411-437.
Indication: Bladder cancers
- Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: a prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. van der Zee J, Gonzalez Gonzalez D, van Rhoon GC, et al. Lancet 2000;355:1119-1125.
- Is hyperthermia combined with radiotherapy adequate in elderly patients with muscle-invasive bladder cancers? Thermoradiobiological implications from an audit of initial results. Datta NR, Eberle B, Puric E, et al. Int J Hyperthermia 2016 (in press) DOI: 10.3109/02656736.2015.1132340.
- Hyperthermia and radiotherapy in bladder cancer. Snider III J, Datta NR, Vujaskovic Z. Int J Hyperthermia 2016 20; 1-9.
- Quadrimodal treatment of high-risk T1 and T2 bladder cancer: transurethral tumor resection followed by concurrent radiochemotherapy and regional deep hyperthermia. Wittlinger M, Rödel CM, Weiss C, et al. Radiother Oncol. 2009 Nov;93(2):358-63.
- Thermoradiation in muscle invasive bladder cancer (MIBC): A Valuable therapeutic option for elderly or inoperable patients. Puric E, Datta NR, Eberle B, et al. ESHO 2017, Athens, 23-25 June 2017, p 38-39.
- Thermoradiotherapy in muscle invasive bladder cancer (MIBC) : a valuable therapeutic option for elderly or inoperable patients. Puric E, Datta NR, Eberle B, et al. SASRO 2017, St. Galen, 8-10 June 2017.
- Thermo-Radiotherapy in bladder cancer is a promising option in patients unfit for cystectomy or chemo-radiotherapy. Stutz E, Eberle B, Puric E, et al. SASRO 2018.
- A Pilot Study of Radiotherapy and Local Hyperthermia in Elderly Patients With Muscle-Invasive Bladder Cancers Unfit for Definitive Surgery or Chemoradiotherapy. Datta NR, Stutz E, Puric E, et al. Front Oncol 2019;9:889.
Indication: Rectal/Anal canal cancer
- Chemoradiotherapy combined with intracavitary hyperthermia for anal cancer: Feasibility and long-term results from a phase II randomized trial. Kouloulias V, Plataniotis G, Kouvaris J, et al. Am J Clin Oncol 2005;28:91-9.
- Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: a prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. van der Zee J, Gonzalez Gonzalez D, van Rhoon GC, et al. Lancet 2000;355:1119-1125.
- Adjuvant VHF therapy in locally recurrent and primary unresectable rectal cancer. Trotter JM, Edis AJ, Blackwell JB, et al. Australas Radiol 1996;40:298-305.
- An alternative treatment of anal squamous cell carcinoma: Combined radiotherapy and chemotherapy. You YT, Wang JY, Changchien CR, et al. J Surg Oncol 1993;52:42-5.
- Thermoradiotherapy of patients with locally advanced carcinoma of the rectum. Berdov BA, Menteshashvili GZ. Int J Hyperthermia 1990;6:881-90.
- Long-term local control and survival after preoperative radiochemotherapy in combination with deep regional hyperthermia in locally advanced rectal cancer. Gani C, Schroeder C, Heinrich V, et al. Int J Hyperthermia. 2016;32(2):187-92.
- Chemoradiotherapy and concurrent radiofrequency thermal therapy to treat primary rectal cancer and prediction of treatment responses. Shoji H, Motegi M, Takakusagi Y, et al. Oncol Rep. 2017 Feb;37(2):695-704.
- Selecting patients for hyperthermia combined with preoperative chemoradiotherapy for locally advanced rectal cancer. Kim SW, Yea JW, Kim JH, Gu MJ, Kang MK. Int J Clin Oncol 2018;23:287-297.
- External validation of a rectal cancer outcome prediction model with a cohort of patients treated with preoperative radiochemotherapy and deep regional hyperthermia. Zwirner K, Bonomo P, Lamprecht U, Zips D, Gani C. Int J Hyperthermia 2018;34:455-460.
- Chemoradiotherapy with and without deep regional hyperthermia for squamous cell carcinoma of the anus. Ott OJ, Schmidt M, Semrau S, et al. Strahlenther Onkol 2019;195:607-614.
Indication: Soft tissue sarcoma
- Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: a randomised phase 3 multicentre study. Issels RD, Lindner LH, Verweij J, et al. Lancet Oncol 2010;11:561-570.
- Regional deep hyperthermia for salvage treatment of children and adolescents with refractory or recurrent non-testicular malignant germ-cell tumours: An open-label, non-randomised, single-institution, phase 2 study. Wessalowski R, Schneider DT, Mils O, et al. Lancet Oncol 2013;14:843-52.
- Could hyperthermia with proton therapy mimic carbon ion therapy? Exploring a thermo-radiobiological rationale. Datta NR, Puric E, Schneider R, et al. Int J Hyperthermia 2014;30:524-530.
- Effect of Neoadjuvant Chemotherapy Plus Regional Hyperthermia on Long-term Outcomes Among Patients With Localized HighRisk Soft Tissue Sarcoma: The EORTC 62961-ESHO 95 Randomized Clinical Trial. Issels RD, Linder LH, Verweiji J, et al. JAMA Oncol. 2018 Feb 15;4:483-492.
- Early results of spot scanning proton therapy with hyperthermia in large inoperable sacral chordoma. Walser M, Datta NR, Puric E, et al. ESTRO Barcelona, Radiother Oncol 2018; 127 (suppl 1): s882-83.
- Hyperthermia combined with proton therapy in inoperable sacral chordomas: First clinical experience and early results. Puric E, Datta NR, Walser M, et al. ESHO 2018, 16-18 May 2018.
- First case report of concurrent proton therapy with hyperthermia in a large extra-abdominal desmoid tumor. Stutz E, Murray F, Puric E, et al. SASRO 2018.
- Large Malignant Fibrous Histiocytoma Treated with Hypofractionated Proton Beam Therapy and Local Hyperthermia. Iizumi T, Shimizu S, Numajiri H, et al. Int J Part Ther 2019;6:35-41.
- Early results and volumetric analysis after spotscanning proton therapy with concomitant hyperthermia in large inoperable sacral chordomas. Tran S, Puric E, Walser M, et al. Br J Radiol 2019:20180883.
- Neoadjuvant chemotherapy plus radiation versus chemotherapy plus regional hyperthermia in high-grade soft tissue sarcomas: a retrospective comparison. Zschaeck S, Wust P, Melcher I, et al. Int J Hyperthermia 2018;35:1-9.
- Radiotherapy and hyperthermia with curative intent in recurrent high risk soft tissue sarcomas. Eckert F, Braun LH, Traub F, et al. Int J Hyperthermia 2018;34:980-987.
Indication: Pancreas Carcinoma
- Gemcitabine and cisplatin combined with regional hyperthermia as second-line treatment in patients with gemcitabinerefractory advanced pancreatic cancer. Tschoep-Lechner KE, Milan V, Berger F, et al. Int J Hyperthermia 2013; 29: 8-16.
- Phase II trial of combined regional hyperthermia and gemcitabine for locally advanced or metastatic pancreatic cancer. Ishikawa T, Kokura S, Sakamoto N, et al. Int J Hyperthermia 2012; 28: 597-604.
- Regional hyperthermia combined with chemoradiotherapy in primary or recurrent locally advanced pancreatic cancer : An open-label comparative cohort trial. Maluta S, Schaffer M, Pioli F, et al. Strahlenther Onkol 2011;187:619-25.
- Preclinical and clinical aspects of carboplatin and gemcitabine combined with whole-body hyperthermia for pancreatic adenocarcinoma. Bakshandeh-Bath A, Stotlz AS, Homann N, et al. Anticancer Res 2009; 29: 3069-3078.
- The effect of the combination therapy of hyperthermia and gemcitabine for the treatment of advanced inoperable pancreatic cancer. Takagi T, Kokura S, Ishikawa T, et al. 10th International Congress on hyperthermia Oncology, Munich, Germany, 9 – 12 April 2008, p. 50 (Abstract).
- Comparison of concomitant gemcitabine chemotherapy and local hyperthermia, gemcitabine monotherapy and local hyperthermia monotherapy for inoperable progressive pancreatic cancer. Yasuda M, Kondo M, Kokura S, et al. J Clin Oncol, 2008, 26: 15772 (abst).
- Intraoperative hyperthermia in conjunction with multi-schedule chemotherapy (pre-, intra- and post-operative) by-pass surgery and postoperative radiotherapy for the management of unresectable pancreatic adenocarcinoma. Kouloulias VE, Kouvaris JR, Nikita KS, et al. Int J Hyperthermia 2002;18: 233-52.
- „HEATPAC“ – a phase II randomized study of concurrent thermochemoradiotherapy versus chemoradiotherapy alone in locally advanced pancreatic cancer. Datta NR, Pestalozzi B, Clavien PA, et al. Radiat Oncol. 2017 Nov 21;12(1):183.
- A phase II randomized study of concurrent hyperthermia and chemoradiotherapy vs chemoradiotherapy alone in locally advanced pancreatic cancer (HEATPAC): first information and call for participation. Datta NR, Pestalozzi B, Clavien P, et al, HEATPAC Trial Group. (ClinicalTrials.gov Identifier: NCT02439593) ESHO 2017, Athens, 23-25 June 2017, p 56-57.
Indication: Deep seated bony metastasis
- Comparing the effectiveness of combined external beam radiation and hyperthermia versus external beam radiation alone in treating patients With painful bony metastases: A Phase 3 Prospective, Randomized, Controlled Trial. Chi MS, Yang KL, Chang YC, et al. Int J Radiat Oncol Biol Phys. 2018 Jan 1;100(1):78-87.
- Evaluating the effectiveness of combined radiotherapy and hyperthermia for the treatment response of patients with painful bony metastases: A phase 2 clinical trial. Ariyafar T, Mahdavi SR, Geraily G, et al. J Therm Biol 2019;84:129-135.
Contributions by KSA to promote hyperthermia in National and International scientific forums (2018 -2019)
- Awarded “European Society of Hyperthermic Oncology (ESHO) Member of Merit”. December 2019. (Prof. N. R. Datta)
- Elected Board Member, European Society of Hyperthermic Oncology (ESHO). (Prof. N. R. Datta).
- Publications related to hyperthermia (2018-19): Full length articles in peer-reviewed journals: 7
- Keynote presentations at the Annual Conference of the European Society of Hyperthermic Oncology (ESHO). Warsaw, 2019. (Prof. S. Bodis, Prof. N. R. Datta).
- Keynote presentations at the Annual Conference of the International Conference of Hyperthermia Oncology (ISHO). 2018 (Budapest) and 2019 (Thessalonski). (Prof. S. Bodis, Prof. N. R. Datta).
- Coordinated the proposal for first ever multi-centric clinical trial proposal meeting in hyperthermia, endorsed by ESHO. Nov 2019, Amsterdam. (Prof. S. Bodis).
- One of the main collaborators for the EU Grant proposal to develop Hyperthermia boosting the effect of Radiotherapy (HYPERBOOST): Decision awaited.
- Submitted proposal for a Panel session on Hyperthermia at the forthcoming American Society for Therapeutic Radiaology and Oncology (ASTRO). 2019: Decision awaited.
- Conducted a Educational Session at the Scientific Association for Swiss Radiation Oncology (SASRO) conference. 2019 entitled, “Hyperthermia: Overview of Clinically Validated Indications”.
- Invited to propose and conduct a Special Sessions on “Hyperthermia” at the forthcoming Scientific Association for Swiss Radiation Oncology (SASRO) conference. 2020.
 Hyperthermietumorboard
Hyperthermietumorboard
 Hyperthermietumorboard
HyperthermietumorboardIm Rahmen des schweizer Hyperthermienetzwerkes beteiligt sich das ZIO am wöchentlichen Hyperthermietumorboard.
Wöchentlich am Montag, 16:30 Uhr
Direkt zur Anmeldung >
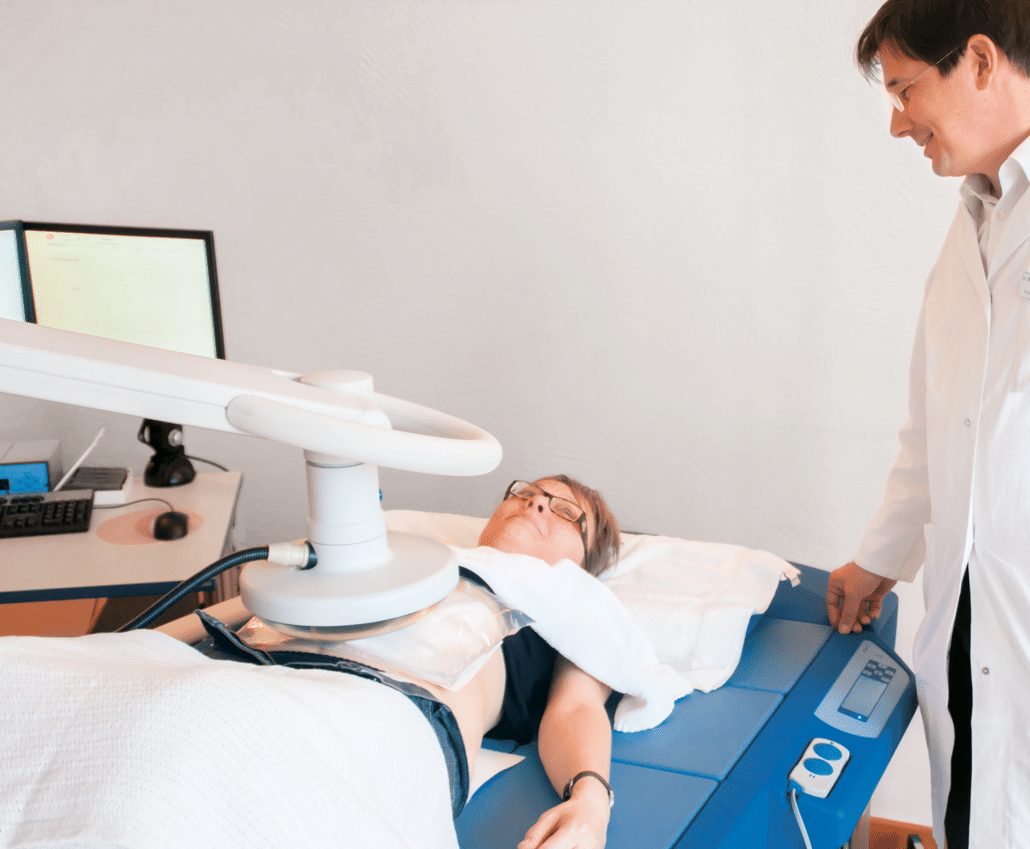
Lokale Tiefenhyperthermie
Mit der lokalen Tiefenhyperthermie können lokale und regional begrenzte Tumoren behandelt werden. Dabei wird durch sogenannte Kurzwellenstrahlung für die Dauer von 50 Minuten eine Temperatur von 42 bis 44 Grad Celsius erzeugt. Diese Hitze löst verschiedene Reaktionen in der Krebszelle aus, die zu ihrem Untergang führen können. Gesundes Gewebe wird dabei nicht geschädigt.
Weitere Infos
Die Behandlung erfolgt auf einem Therapiebett, das mit Auflage-Kacheln und einer Kachel-Elektrode versehen ist. Die Kachel-Elektrode und eine weitere Elektrode werden gezielt an der zu behandelnden Körperregion positioniert. Die Körperpartie zwischen den beiden Elektroden wird während der Therapie von Radiowellen mit einer Frequenz von 13,56 Megahertz durchströmt. Vor und während der Behandlung können über ein Display diverse Einstellungen vorgenommen, gesteuert und verändert werden. Ausserdem überwacht ein Computer während der Behandlung kontinuierlich alle sicherheitsrelevanten Parameter und dient zur ausführlichen Dokumentation. Die Behandlung kann jederzeit vom Patienten unterbrochen werden. Im Gegensatz zu Operation, Chemothera-pie und Strahlentherapie ist die Hyperthermie nahezu nebenwirkungsfrei. Es kann sogar sein, dass Sie sich während der Behandlung sehr wohl fühlen.
Im Einzelfall kann die Behandlung eines Tumors erschwert sein, der sich in unmittelbarer Nähe zu einem Hüft- oder Kniegelenksersatz befindet. Patienten mit einer gestörten Temperaturwahrnehmung können nur mit spezieller Überwachung behandelt werden. Für Patienten mit Herzschrittmachern und anderen Schrittmacher-Elektroden ist die Therapie mit lokaler Tiefenhyperthermie leider nicht möglich.
{kind=link}
{kind=link}
{kind=link}
Moderate Ganzkörper-Hyperthermie
Der gesunde Körper reagiert auf krank machende Reize mit Temperaturerhöhungen bis zu hohem Fieber. Entsprechend kann auch die künstliche Erhöhung der Körpertemperatur die blockierten Selbstheilungskräfte bei chronischen und bösartigen Erkrankungen nachhaltig anregen. Bei der moderaten Ganzkörper-Hyperthermie erfolgt die Wärmezufuhr durch Infrarotstrahlung mit einem hohen Anteil an wassergefiltertem Infrarot A. Diese Strahlung dringt so tief in das Gewebe und die Unterhaut ein, dass die dabei freigesetzte Wärme vom Blut aufgenommen und im ganzen Körper verteilt werden kann. Dies geschieht über eine gleichmässige und hautverträgliche Bestrahlung.
Weitere Infos
Wann wird die Ganzkörper-Hyperthermie eingesetzt?
- Ergänzende Anwendung bei Krebserkrankungen
- Fibromyalgiesyndrom und chronisches Müdigkeitssyndrom
- Rheuma
- Chronische Hauterkrankungen, z.B. Schuppenflechte und weitere
Wie erfolgt die Behandlung?
Die moderate Ganzkörper-Hyperthermie besteht aus drei Phasen:
- Aufwärmphase von ca. 90 bis 120 Minuten, in der die Körpertemperatur ansteigt
- Wärmestauphase von ca. 120 Minuten, in der das Körpertemperaturmaximum erhalten werden soll
- Entlastungsphase, in der sich die Körpertemperatur wieder normalisiert
{kind=link}
{kind=link}
{kind=link}